
Why Doctors Don’t See Withdrawal
Severe antidepressant withdrawal is often hidden in plain sight. Here's why most clinicians don't recognise it – and why I wouldn't have either until it happened to me.

There is an apocryphal story of a university prank that goes something like this: a group of university students go up to some workmen digging up a road, and tell them that a group of university students pretending to be policemen are coming towards them as part of a prank. Then they go round the corner and tell a group of policemen a version of the same story: just down the street is a group of university students pretending to be workmen and digging up the road for a joke. In accordance with the universal laws of slapstick comedy, the whole thing naturally degenerates into a fistfight when workmen and policemen finally meet. Each side is convinced that they are the wounded party, and that the other side is acting in bad faith.

It strikes me that debate about antidepressant withdrawal within psychiatry has become similarly farcical, bifurcated into two groups that often view each other with deep suspicion and mistrust. As a doctor who works in psychiatry with personal experience of antidepressant withdrawal, I am in the unique and often uncomfortable position of having been, metaphorically speaking, both a ‘workman’ and a ‘policeman’. I have been on both sides of the increasingly unfunny ‘prank’ that is current deprescribing discourse, and as such I’d like to try to sketch out some of the misconceptions that I think are making this discussion more conflictual than it needs to be.
Group #1 ‘The Workmen’: Mainstream psychiatrists
The first group caught up in the ‘prank situation’ are mainstream psychiatrists. This group, populated by what are probably the majority of mental health professionals, regards antidepressant withdrawal as a relatively minor issue, as it is characterised in most guidelines and educational programs around the world. They grant that it is an issue worthy of some attention, and that tapering perhaps ought to be done more carefully than in the past (with much debate about what ‘more carefully’ actually entails). Nevertheless, they see antidepressant withdrawal as a relatively small problem, especially in the context of a class of drugs whose benefits outweigh their downsides for the majority of patients.
From the perspective of Group #1, antidepressant withdrawal amounts to a minor clinical footnote that has been inflated out of all proportion by the harmed patients and critical professionals in Group #2. Social media, ‘anti-psychiatry’ activism, and a small but vocal group of clinicians and patients are held responsible for creating a mountain out of what should be, in Group #1’s view, only a modestly sized mole hill.
The impression formed of such Group #2 patients is that they are equivalent to ‘disgruntled former employees’, people unhappy with their lot in life who are placing the blame for their problems on their drugs or clinicians. Or they are perceived as ideologically opposed to psychiatry in the same way that some people are seen as ideologically opposed to vaccines – that is, for reasons that go far beyond what is warranted by the facts.
The critical clinicians and researchers who are part of Group #2 are assumed by members of Group #1 to be motivated by a suspect desire to bring psychiatry into disrepute, for reasons that presumably include a desire to make money or achieve fame, or simply because they enjoy being controversialists. This view is exemplified by Professor McGorry, a luminary of Australian psychiatry. On social media, Professor McGorry has compared my commentary on antidepressant withdrawal to an unbalanced oncologist constantly posting about the downsides of chemotherapy, without ever acknowledging its benefits. (I won’t get into it here but of course the situation with chemotherapy which is used successfully to treat a disease with an often high mortality rate is completely different to antidepressants which are used to treat an extremely common condition, with a very low mortality rate, with much more marginal benefits. Not to mention that patients and doctors are well aware of the risks of chemotherapy, compared to widespread downplaying of antidepressant adverse effects, especially withdrawal effects).
But the truth is that if I hadn’t gone through antidepressant withdrawal myself, I am certain that I would be squarely in Group #1. I think my record speaks for itself.
I did my PhD at King’s College London, studying the neurobiology of depression and the action of antidepressants. While I was there, my GP at the time commented that I seemed to be doing well with everything and suggested I consider discontinuing the antidepressant I had been on for so many years. I was outraged! I told her that if I was doing well it was probably because of the antidepressant, and followed it up with a sermon about my credentials. I was a trainee psychiatrist actually, had just spent two years studying how antidepressants work, and she should reflect on how reckless it was to suggest stopping taking these useful drugs.
Another example of how much my sympathies were aligned with Group #1 came while working in Australian youth mental health services (Headspace - as it happens, set up by Prof McGorry): I attended a workshop given by a man who had been diagnosed with treatment-resistant schizophrenia. He described receiving every pharmaceutical treatment psychiatry had to offer, including clozapine, and electroconvulsive therapy. He eventually recovered through trauma-focused therapy, peer support, and coming off psychiatric drugs. After the lecture advocating for a trauma-informed approach I stood up, incensed, and told him he was obviously an outlier, unrepresentative of the huge numbers of people who needed these drugs. I remonstrated him for advocating an approach that would lead to suicides and terrible consequences.
Years later, I can still remember the quivering outrage in my voice as I ardently defended psychiatric practice in the face of what I believed at the time were entirely unreasonable critiques. I hear that same outrage today in the voices of people in Group #1, when exposed to discussion of antidepressant withdrawal (and related topics).
Group #2 The ‘Policemen’: Harmed patients and critical mental health professionals
Group #2, the ‘policeman’ in our prank, consists largely of patients who report severe withdrawal effects and other iatrogenic problems from psychiatric drugs, together with the clinicians and researchers who work with this population.
It would be pointless to pretend that I am not firmly in Group #2 today. I won’t rehash here how I came close to losing my life during withdrawal from an antidepressant, something I have written about elsewhere. Needless to say, I am not in much of a position to doubt that withdrawal from psychiatric drugs can cause akathisia, suicidality and extreme mental and physical suffering as I have lived through this myself. My clinical work and research are now entirely focused on helping people safely stop no longer needed psychiatric drugs, especially antidepressants, and supporting people suffering protracted withdrawal syndromes. I have written the Maudsley Deprescribing Guidelines which is a guide on how to stop psychiatric drugs carefully.
The harmed patients and critical professionals in Group #2 tend to locate members of Group #1 somewhere along a spectrum from naïvely ignorant to wilfully blind, or in some cases actively malicious. But as someone who has been on both sides of this ‘prank’, I don’t think it’s that simple.
The ‘Prank’- Why doctors don’t see withdrawal
If I had encountered the debate about antidepressant withdrawal before my own discontinuation experience, I would have struggled to believe the claims of harmed patients in Group #2.
If someone had told me then that antidepressant withdrawal could cause months of panic attacks, dissociation, tinnitus, balance problems, muscle pain, akathisia and cognitive impairment, and that some people needed to taper over years down to micro-doses to avoid these problems, I suspect I too would have regarded such claims as exaggerated, internet-driven, and perhaps reflective of a relatively small group of distressed or ideologically motivated people.
Like so many psychiatrists today, I think I would have accepted commentators like Awais Aftab as representing the sensible centre of this debate - acknowledging the limitations of psychiatric practice and the existence of withdrawal effects, whilst not going overboard and throwing the antidepressant benefits baby out with the withdrawal bathwater. If I had come across studies (double-blinded, randomised studies no less) which repeatedly found that withdrawal effects occur to most long-term users I would have been very confused.
The main reason for this is that in years of psychiatric training and clinical practice I had only seen one case of antidepressant withdrawal – so I have great sympathy when I hear clinicians say something similar.
In retrospect, this is because it is difficult for doctors to see something that they haven’t been taught to look for.
As someone who has spent time on both sides of this fistfight, I don’t think wilful blindness or malevolence explains the views of the mainstream psychiatrists in Group #1. Rather, there are a number of structural and conceptual factors that explain why antidepressant withdrawal is so often missed or misinterpreted. In terms of our analogy, these factors might be thought of as the students pulling the prank in the first place, sewing discord between the unsuspecting workmen and innocent policemen in Groups #1 and #2.
So, why don’t doctors see withdrawal?
1. Drugs are rarely stopped without being replaced by another drug
Looking back on my clinical practice before encountering withdrawal first-hand, I have a hard time recalling occasions where long-term psychiatric drugs were stopped entirely without being replaced by another drug. Sometimes a recently started drug was stopped if a patient reacted badly to it, but because of the short duration of exposure this was never very likely to cause withdrawal effects. Sometimes drugs were switched because they were thought not to be effective or because they were causing troubling side effects, but complete discontinuation was relatively uncommon. When dose reductions did occur they tended to be quite modest and made from higher starting doses, where dramatic withdrawal effects are less likely to emerge. Additionally, if a patient is on multiple drugs, as so many patients in secondary services are, then stopping one drug is likely to be buffered by the other drugs and so minimise the emergence of withdrawal effects.
Keeping patients on psychiatric drugs long-term makes sense within the logic of conventional psychiatric practice and training. Most patients in public psychiatric settings are seen to have severe, recurrent or high-risk conditions and clinicians are therefore reluctant to “rock the boat”. If someone has been stable for years on medication, stopping it entirely can feel risky for the clinician responsible for their care, and often for the patients or their families as well.
In primary care meanwhile, time pressures and competing priorities often mean that deprescribing falls rather low down the list. There is some objective evidence for this pattern. In one Dutch study of antidepressant discontinuation, only 8% of people in the control group (clinical practice as usual without any intervention) without an ongoing indication for antidepressants stopped them in a given year.
If long-term drugs are rarely stopped outright, clinicians will naturally see relatively little withdrawal.
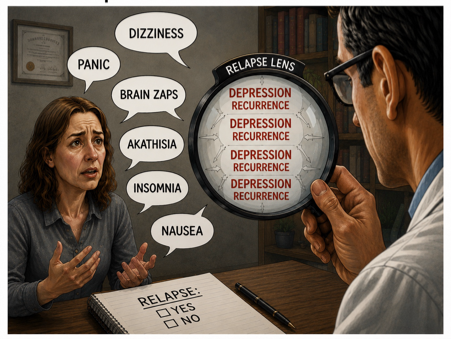
2. Withdrawal is mistaken for relapse
This is probably the single biggest reason that doctors fail to recognise withdrawal.
(i) The primacy of relapse
Relapse looms very large in clinicians’ minds. It is no exaggeration to say that relapse prevention is one of the central organising principles of conventional psychiatric practice (after managing acute crises). Psychiatrists spend years hearing lectures about relapse after medication cessation and seeing firsthand in emergency departments patients who deteriorate after stopping medication (and who often improve when this medication is re-started). Preventing people from becoming unstable again is, understandably enough, one of the key aims of the profession. This becomes the lens through which clinicians view clinical presentations.
(ii) Minimisation of withdrawal
Withdrawal, by contrast, receives remarkably little attention. My friends and colleagues are sick of hearing me make this joke, but the first lecture I ever heard about stopping psychiatric drugs was one I gave myself.
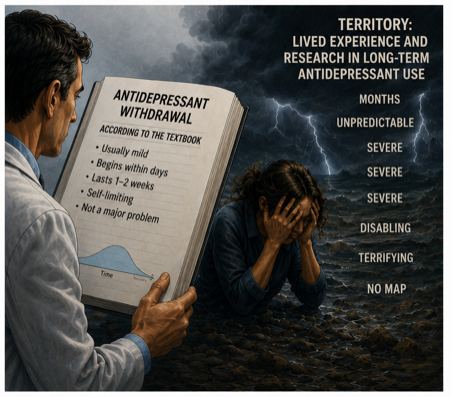
Again, this neglect is understandable given the context. The drug industry conducted studies of antidepressant discontinuation mostly following 8 to 12 weeks of antidepressant exposure. These studies generally found withdrawal to be ‘mild and brief’, lasting one or two weeks, and these widely amplified studies heavily shaped guidelines and educational materials for decades.
Not only did these studies involve relatively short-term antidepressant use, which is simply not comparable to the years and decades of use typical for the average real-life patient, they often were not primarily designed to detect withdrawal symptoms. They certainly weren’t capable of capturing experiences of prolonged or delayed withdrawal.
Some of these studies have recently been repackaged into newer meta-analyses published in high profile journals. Though the results are dressed up to give the appearance of novel, high quality work, they are still critically flawed due to the poor quality of the studies that went into them. The end result of these failures has been a generation of clinicians taught that withdrawal is transient and relatively benign.
So when someone presents after reducing medication with severe anxiety, insomnia, agitation, dizziness, cognitive problems or emotional instability, it isn’t surprising that relapse springs to mind first while withdrawal barely enters the differential diagnosis. If the symptoms persist for long periods (explained here), then clinicians educated to believe that withdrawal should last only a week or two will naturally believe that there must be something else going on.
I remember once being called by a baffled physician from a medical ward about an elderly man who had suddenly become severely agitated and suicidal. He had apparently been mentally stable only days earlier. Eventually his daughter realised that his duloxetine had accidentally been omitted from his medication chart after admission to hospital.
My supervising consultant and I briefly considered delirium and agitated depression before eventually concluding, somewhat uncertainly, that this might actually be antidepressant withdrawal. The duloxetine was restarted and the symptoms settled relatively quickly. Even at the time, this presentation struck me as surprisingly extreme.
Prior to my own withdrawal experience, I would have said that this was the only time I had encountered withdrawal from a psychiatric drug in all my years of clinical practice.
Since experiencing severe withdrawal myself, however, I have had disturbing flashbacks to former patients. Patients who arrived in emergency departments profoundly agitated after abruptly stopping antipsychotics or other drugs, sometimes pacing in a way that seems, in retrospect, highly suggestive of withdrawal-induced akathisia. Patients whose notes described years of stability derailed by sudden behavioural chaos after drug cessation – chaos of a kind far more extreme and debilitating than anything experienced in previous episodes. I recall one patient who would appear at the in-patient unit I worked at every few weeks after repeatedly stopping lithium. He had a martial arts background and would be frighteningly agitated on presentation. Month after month he had his lithium re-started, and month after month he came back suffering what I now recognise was very plausibly withdrawal.
At the time I interpreted these presentations automatically through the framework of relapse, as did everyone else around me. Withdrawal as a concept was totally foreign to me – it would never even have crossed my mind. Not because I was uncaring or incompetent but because it had never really been presented to me as something I should actively be looking for.
Ultimately, it is difficult to see what you have not really been taught to see.
(iii) Characterisation of withdrawal as physical symptoms only
When withdrawal effects are mentioned in medical education and academic studies, they tend to be characterised as predominantly physical symptoms. This is the final thing that causes clinicians to misperceive withdrawal effects as relapse. ‘Brain zaps’, dizziness and headache for example are emphasised. So when people walk into an office complaining of panic and low mood, the doctor’s mind snaps automatically to relapse. But in fact, emotional withdrawal symptoms are more common than physical ones.
We are all familiar with the emotional instability that accompanies other withdrawal states. Think of the misery of a hangover caused by drinking too much alcohol, or the irritability caused by nicotine withdrawal when quitting smoking. As a psychotropic drug that has profound effects on the brain, it is hardly surprising that antidepressant withdrawal should include so many emotional symptoms, and indeed an analysis of more than a thousand people suffering from withdrawal effects found that anxiety, low mood and agitation were in the top five most common symptoms. This held true for patients who had been prescribed antidepressants for conditions unrelated to mental health. These were people taking the drugs to treat conditions like pain or insomnia, people who had never experienced clinical anxiety or depression prior to discontinuing the drugs and who therefore had no underlying mental health condition to ‘relapse’ to in the first place.
Due to the framing of withdrawal as largely physical, any report of emotional symptoms is likely to quickly send clinicians down the path of erroneously diagnosing relapse. Influential clinicians have even gone so far as to say that if symptoms register on a depression rating scale then they must be relapse by definition. Given how non-specific many of the symptoms such checklists capture (low mood, trouble sleeping, anxiety) that are also common withdrawal effects, his is a bit like saying that anything that fits into a jar labelled ‘apples’ must be an apple: not terribly convincing, but indicative of the fact that psychiatrists are taught to perceive emotional symptoms through the prism of relapse.
3. The familiarity of withdrawal symptoms
While I was tapering, I would reduce my dose of escitalopram by around 10% and then spend several weeks suffering poor sleep, low mood, exhaustion, dissociation and a feeling that I have best heard described as ‘having cotton wool in your head’. A few weeks after I’d made the reduction these symptoms would settle.
Nonetheless, one of the most confusing things about withdrawal for me personally was the strange ring of psychological familiarity that accompanied some of these symptoms. At various points I became convinced I was relapsing. I remember panicking and torturing myself, thinking, “Maybe I really do need antidepressants. Perhaps it was a terrible mistake to think I could come off these drugs. What on earth were you thinking Horowitz?”
Eventually my long-suffering sister, tired of listening to my repetitious whinging, insisted that I record a video message to myself explaining that every dose reduction reliably produced a temporary period of despair and disorientation that nonetheless always passed. Although the symptoms sometimes bore the familiar imprint of my existentially anxious, Woody Allen-esque personality, they were nonetheless physiological symptoms of antidepressant withdrawal, not proof that I ‘needed’ the drug. That video became surprisingly important. I played it to myself on repeat during the darker parts of my taper.
I eventually came to see the process of withdrawal as being a bit like a video I saw on the internet of people diving down a storm-water drain. This drain looped underground before eventually resurfacing. For the diver in the middle of that dark tunnel deep beneath the earth, it was easy to be overwhelmed by panic and claustrophobia. You might die down there! But if you kept swimming, you would emerge from the murky depths and resurface safely.
Low mood is, in many respects, a fairly generic human state. The low mood you experience after a break-up, or disappointment, or during a hangover have much in common. There might be more sharp anguish in a breakup and more dry mouth in a hangover, but in many ways our emotional states are somewhat generic to each of us, no matter what their cause.
In such states, we all express typical patterns of emotions and thoughts that are unique to us as individuals. For example, if everyone reading this essay (all 12 of you!) drank a litre of coffee you would all become anxious, but the particular flavour of anxiety experienced by each person would differ according to that person’s particular fears, vulnerabilities and habits of thought. If you tend to worry about your physical health, then your caffeine induced anxiety will probably centre on worries about your heart rate. If, like me, you worry about your receding hairline, then losing your hair is what might spring to mind when you get the caffeine jitters. Antidepressant withdrawal appears to work similarly: although induced by chemicals, the symptoms are filtered into idiosyncratic and oddly familiar shapes by the idiosyncratic mind of the person experiencing them.
For all these reasons it is easy for people to mistake withdrawal effects for relapse. Combined with a tendency for clinicians to automatically interpret deterioration after stopping medication as relapse, this creates a powerful pull towards that diagnosis. What eventually helped me distinguish withdrawal from relapse in my case was noticing that symptoms that had never accompanied feeling low in the past were always present with it – derealisation, dissociation, profound cognitive fog, and that peculiar “cotton wool in the head” sensation. These symptoms tracked alongside my dips in mood, and many patients describe something similar. There are also others who report that their withdrawal symptoms were completely novel, and felt nothing like their original condition. But for many people the overlap is substantial enough that relapse becomes the obvious interpretation, both to themselves and to clinicians.
4. The symptoms themselves sound implausible
If I had encountered online withdrawal forums before my own experience, I suspect I would have dismissed many of the reports as implausible. Baylissa Frederick, a counsellor who went through withdrawal herself, has described this as ‘the unbelievability factor’.
People describe being bed bound for months or developing severe panic attacks after stopping antidepressants originally prescribed for stress or grief. They experience dizziness, tinnitus, electric shock sensations, muscle spasms, balance problems, visual disturbances and suicidality. Others describe needing years-long tapers down to tiny doses.
To a conventionally trained psychiatrist, much of this sounds extraordinary and difficult to reconcile with ordinary clinical experience. After all, these are medications prescribed to millions of people. Many psychiatrists have prescribed them thousands of times. And most believe they have rarely seen serious withdrawal. Given that background, alternative explanations naturally seem more plausible: psychosomatic symptoms, anxiety, underlying conditions, new-onset psychiatric conditions, functional neurological disorders, somatisation, or even malingering.
Years ago, well before he knew about my involvement in withdrawal research, a very senior (and knighted) professor of psychiatry said to me in the corridors of the Royal Society for Medicine, “These neurotic people are just attributing their problems to the drugs.”
I asked, politely, “Headaches, dizziness, panic attacks…you think these are all part of the underlying disorder?”
“Exactly!” he replied emphatically, “Many people don’t understand how many physical symptoms are part of depression and anxiety. People’s mood comes out in all sorts of peculiar ways.”
“Even brain zaps?” I asked dubiously.
“Yes, even them” he replied, nodding soberly.
Unfortunately, further questioning on my part led to what the British might euphemistically call a ‘deterioration’ in my relationship with this particular colleague. I understand why he believed what he believed and, sadly, I suspect I would once have believed it too.
5. Patients often restart medication before clinicians see the full syndrome
While reinstatement doesn’t always work, withdrawal symptoms frequently improve after reinstating the drug. This creates a kind of feedback loop. A patient stops medication, deteriorates, restarts the drug, and then improves. Both patient and clinician can then quite reasonably conclude that the medication had been successfully treating an underlying illness rather than recognising the possibility of withdrawal. The withdrawal syndrome effectively disappears before it can be clearly observed.
I’ve covered this above from the clinician perspective and touched on it for patients, but the other aspect of this is that patients themselves have also been immersed in ideas about relapse. Many have been told they have a lifelong condition, that is caused by a ‘chemical imbalance’ and so when they experience a bump in their mental stability from withdrawal they too jump to the conclusion that they have relapsed. This is where narratives about a ‘chemical imbalance’ and that withdrawal is mild and brief and not very common intersect. I realise now when I look back that over the years when I have tried to stop my antidepressant not in the intentional way I did 10 years ago with catastrophic consequences but more casually, I have often interpreted the dip in my mood a few weeks later as evidence that I needed to get back on the drug – this must occur to millions of people.
6. Delayed onset obscures causality
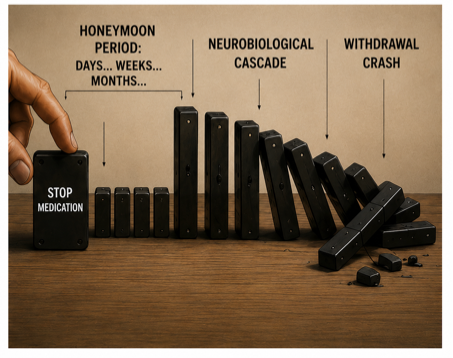
Withdrawal does not always begin immediately. Many clinicians have been taught that if a drug leaves the body within days, symptoms emerging weeks later cannot plausibly be related to discontinuation. We don’t understand why some patients experience delayed onset withdrawal, but there are now studies finding that many patients have withdrawal delayed by several weeks after stopping their drug – with one study finding that one in six patients have onset more than 4 months after stopping. In other words, although this study may have captured patients who are not representative of wider users (it was from a peer support group of people experiencing withdrawal) it make the point that symptoms onsetting weeks after drug cessation is possible. Delayed onset of biological effects is not unusual: it is generally accepted for antidepressant action and it is also observed in the onset of tardive dyskinesia months after antipsychotics are ceased.
When I first saw such a patient – who had ceased an antidepressant with minor problems and then presented 4 months later with brain zaps, headaches and dizziness - I was quite confused by the presentation. But I have now seen dozens of such patients. While there is minimal research on what is happening in withdrawal, it seems likely that this process involves a cascade of downstream processes that take time to reach a threshold. It is clear that nervous system adaptation (and re-adaptation to the drug not being there) unfolds over much longer timescales than simple drug elimination.
This delayed onset further obscures the connection between stopping medication and later withdrawal symptoms for clinicians. The relationship becomes even harder to recognise when people are taking multiple psychiatric drugs simultaneously, each potentially masking or buffering withdrawal from another.
7. Patients do not return to their doctor out of fear or hopelessness
Many patients who work out for themselves that the issues they have experienced are actually withdrawal and not relapse by reading academic articles or finding online support groups avoid going back to their doctor. Mostly, this is because they find such interactions traumatising. The doctor has told them that it couldn’t be due to withdrawal, it must be their underlying condition or they are somatising in some way or have developed functional neurological disorder. One can see evidence of this sort of response from the psychiatrist influencers on X who constantly make these sort of comments. Patients, deeply sick from withdrawal, cannot tolerate the dismissiveness and gaslighting they experience from clinicians and so end up exiting the health system and relying on peer support sites outside of it. Some of them come back to their prescribers when they heal with academic papers: some doctors pay heed to these but many brush off these sort of approaches, often bristling with wounded professional pride.
8. Cognitive dissonance
Doctors and other prescribers all entered medicine in order to help people. It is upsetting to be confronted with the possibility that your treatment has done more harm than good. I would be deeply upset by this. It is much easier to believe all the other options above: this is relapse, this is a different condition, this person is neurotic, etc. It is easier to shoot the messenger: every day on X you can see a concerted attempt to slaughter messengers. When I stood up to remonstrate the man talking about trauma-informed care at the Headspace in Sydney wasn’t there a part of me that felt myself remonstrated for how I was treating patients? Of course there was.
The Clinician’s Illusion
Taken together, these factors create what might be called a ‘clinician’s illusion’.
Imagine a GP caring for about 2,000 patients.
Perhaps 10% are taking antidepressants at any one time.
If only 6% stop them in a given year, that means that perhaps just 12 patients try to stop annually.
About half will experience no or only mild withdrawal problems and won’t bring it up to their prescriber. The remaining 6 will have moderate or severe problems.
Half of these (three patients) will assume they have relapsed and restart medication immediately, with or without mentioning this to their doctor. There are illustrative stories of celebrities or journalists explaining that they tried to stop their antidepressant but experienced terrible dizziness, headaches and panic attacks. Their message to their followers is: ‘Don’t stop your drugs like I did, look what happened to me - don’t make the same mistake!’. They often say something like, “Coming off these drugs reminded me why I was on them in the first place – I had become complacent because I had been feeling so stable but it was good to be reminded that this is only because I am on medication.” In each case they are mistaking withdrawal symptoms for relapse.
The remaining three patients may present to clinics or emergency departments and are very likely to be told they are relapsing. And most, given the familiarity of their symptoms, their ignorance about withdrawal (if most doctors are not aware of these issues, then most patients will be even less aware) will probably accept that explanation.
Perhaps one of these people will, in the middle of the horror they are going through or perhaps in the aftermath if things settle down on re-instatement, begin to think about how odd it is that they went on a drug because of work stress or bereavement, but now have panic attacks all day and insomnia all night when they try to stop. Perhaps they will go searching for answers online and find, as I did, large groups of people going through similar experiences and academic papers documenting the existence of withdrawal. That one person may well conclude that there is something other than ‘relapse’ going on.
Some of these people turn up to their prescribers’ offices with academic papers clutched in hand, or a copy of the Maudsley Deprescribing Guidelines (I can only apologise for having produced a tome on deprescribing that is the size of a door stop, so massive that doctors no doubt get a sinking feeling in their chests when patients ask them to read it). These people are often dismissed by their doctors, told that withdrawal doesn’t look like this and rarely happens. They are routinely warned to get off social media, in the belief that withdrawal communities are self-perpetuating cesspools of bizarre ideas, comparable to anti-vax communities.
For psychiatrists the numbers are a variation on this them: the average psychiatrist working in public practice might see a few hundred patients in a given year, of which most will be on a psychiatric drug but due to the acuity of most of these patients stopping drugs will not trialed. For the small portion who do stop their medication, many will be on other medications, switch to another drug or have withdrawal mis-perceived as relapse. A psychiatrist in private practice might have patients of lesser acuity and may stop the drugs more often (I more regularly receive emails asking about deprescribing from these sort of psychiatrists) but the same sort of conceptual frame applies in these circumstances.
I often think in these circumstances of how similar the medical profession is to something like the army, with its rigid hierarchy. Infantrymen take commands from lieutenants who in turn take commands from generals, but no soldier of any rank ever takes orders from a civilian. Something similar happens in medicine, where patients have the status of civilians. The hierarchy of the psychiatric profession demands that new information about adverse drug effects be communicated only by professors and professional associations, the medical equivalent of lieutenants and generals. And so too many doctors reject the testimony of their patients. More often than not patients don’t bother returning to their clinicians, both because they are sometimes so sick from withdrawal and because they feel they are met with dismissiveness when they do.
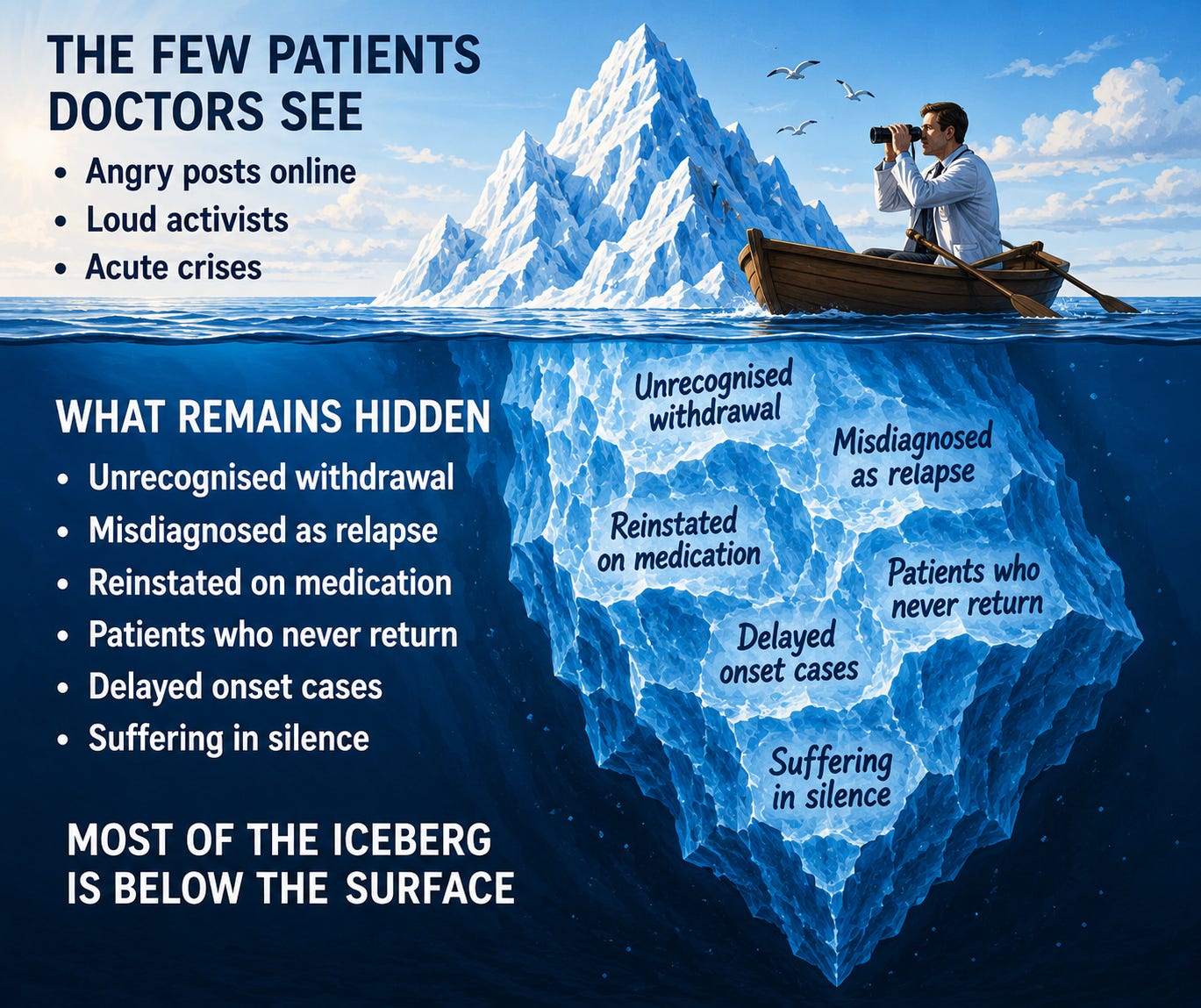
These are the people clinicians eventually encounter online discussing withdrawal. From the clinician’s perspective, they appear to be a tiny but vocally enraged minority. From the patient perspective, they are the visible tip of a much larger iceberg of unrecognised withdrawal. And so the stage is set for the ‘prank’ in our analogy. Like the workmen and policemen set against each other by mischievous students, mainstream psychiatrists engage in farcical fisticuffs with harmed patients and the critical professionals who support them.
None of this requires bad faith, cruelty or wilful blindness on the part of clinicians. It simply requires doctors to interpret symptoms through the conceptual frameworks they have been trained to use and through the kinds of clinical experiences that predominate in routine psychiatric practice. In most cases they fail to recognise withdrawal because they have not been trained to look for it, because the structure of clinical practice often obscures it, and because relapse usually appears, at least initially, to be the more plausible explanation. I understand that mindset intimately because until I experienced withdrawal myself I would almost certainly have shared it too.
The hope that has animated the last few years of my work is that if guidelines could be updated and clinicians were educated about these issues that there would be much less chance for withdrawal to be missed by prescribers. Perhaps naively, I had not anticipated how much energy would be expended to counter this push to educate prescribers from the academic class of psychiatrists and professional institutions. This brings up a hanging question in this extended analogy: who are the students that set this prank up and who perpetuates it? A subject I will tackle in my next blog…
What I wish to say here is that I am sure the average prescriber is giving a good faith account of their experiences when they say they rarely see psychiatric drug withdrawal. It’s just that this view is also completely compatible with about half of long-term users having substantial problems with coming off antidepressants, as many double-blind randomised controlled trials of longer term users show. More senior clinicians tell me that psychiatry is more open to listening to patients than they were back in the day, but I think there is a long way to go.
We have to recall that many important safety signals (such as the consequences of thalidomide during pregnancy and tardive dyskinesia from antipsychotics) were first reported as anecdotal reports. In some ways the very sensible principles of evidence-based medicine have become perverted when randomised controlled trials become the only currency – even when they are short term and not set up to detect the sort of harms that are coming out now in long term users of medication. So I hope that clinicians listen with an open mind to what patients are reporting in their clinics and online rather than expending so much effort to cast aspersions at the motives of patients experiencing severe withdrawal effects.
Great article, and a useful framework for talking with colleagues. As a GP/Rural ED person in Australia, who is at the tail end (I hope) of a lengthy SSRI withdrawal, I find my profession’s addiction to very narrow sources of drug information/guidelines a bit cult-like and anything which might help to gently de-programme them is a boon.
I’m a primary care peds NP who prescribes these meds - more reluctantly and with more informed consent and more discussion from day #1 about not staying on them forever - than in the past. But, still, I prescribe them.
The above - about “than in the past” has admittedly been very much informed by my own experience and what I learned in the process (so much of that from you, so, thank you for your ongoing work in this area!)
I was on Prozac 20mg for a decade. More than one psych NP over those years and never a discussion about tapering off. In fact, the psychiatrist who originally started me on it advised I take it for life “like insulin for a diabetic”. I thought this was his own clever analogy until years later I hear others say they heard the exact same words.
When I asked about tapering off, I was given the standard “drop to 10mg for a week, then stop” advice. I instead decided to taper over 7 weeks and, at the end, it all fell horribly apart. It made no sense to me. I started googling. Exactly what all of us clinicians hate when our patients do. We don’t know what we don’t know. I know now.
I did a hyperbolic taper. 26 months. I finished a few weeks ago. My psych NP believed me… sort of. He said at one point, “I’ve never had a patient struggle to stop Prozac unless they relapsed.” He let me do my thing. Probably partly because he’s a good guy and a reasonable clinician. Probably partly also because I’m also an NP and got a bit more leeway for that.
I gifted him Maudsley about a year in. At the end, I asked him if he’d ever looked at it. He said no. He said “you’ve taught me things also”. Yes, but. Also it was clear he felt my withdrawal had been mild. Um, so not.
I presented at a national peds NP conference in March on deprescribing and will present at a psych NP conference in October. Like you, I’ve sat on both sides of this which I think gives a unique perspective.