
Nonsense Disguised as Nuance: No, the Kalfas Meta-Analysis Doesn’t Prove Antidepressant Withdrawal Is Modest:
A response to Awais Aftab’s commentary on withdrawal, relapse, and clinical complacency

Introduction
In a widely circulated blog post on Psychiatry at the Margins, Awais Aftab offers a detailed interpretation of the recent Kalfas et al. 2025 meta-analysis on antidepressant withdrawal symptoms published in JAMA Psychiatry.
Although he does acknowledge that severe withdrawal occurs and can be a serious problem, and counsels his colleagues not to develop complacency about withdrawal effects, his uncritical acceptance of much of the flawed reasoning and mis-direction in the Kalfas paper (such as the ‘inclusion’ of long-term studies) means that he is perpetuating the very complacency he claims to be warning against.
He frames the study as a blow to the views of what he calls “the critical psychiatry and prescribed harm circles” and claims the findings demonstrate that antidepressant withdrawal is “modest,” statistically detectable but clinically unalarming, and ultimately far less common and severe than critics claim.
Although he accurately points out some of the limitation of the Kalfas paper, including the the short-term nature of the studies included, Aftab nonetheless positions the paper as a welcome correction to “highly-inflated” withdrawal estimates and, burnishing his Genz Z-lingo bonafides, urges anyone “who treats the Davies and Read estimate of antidepressants withdrawal as valid- take the L and move on.”
But far from providing clarity, his interpretation of the Kalfas review suffers from major analytical blind spots—chief among them a fundamental misunderstanding of what the review can (and cannot) tell us about long-term antidepressant use. His argument downplays the significance of the study’s limitations, misrepresents key evidence, and prematurely dismisses the body of work showing that antidepressant withdrawal is both common and sometimes protracted—particularly after long-term use.
Aftab presents himself as sympathetic to patients’ suffering, which I have no doubt he is, but the result of his interventions is to solidify the status quo which misleadingly and systemically dismisses and minimises patients’ concerns.
Here’s where Aftab goes wrong.
1. Short-Term Trials Cannot Be Used to Generalize About Long-Term Antidepressant Use
The entire systematic review conducted by Kalfas captured 50 studies, of which 49 studies contributed data towards meta-analyses. (The only study which didn’t contribute any data to any meta-analysis or any part of the results was the ANTLER study, glossed over by both Aftab and the senior author when defending their paper on Twitter).
However, the main analysis in Kalfas where they concluded that there was an unimportant increase in overall withdrawal effects one week after stopping antidepressants of SMD 0.31 (equivalent to 1.08 extra symptoms on the DESS) was based on only 11 RCTs.
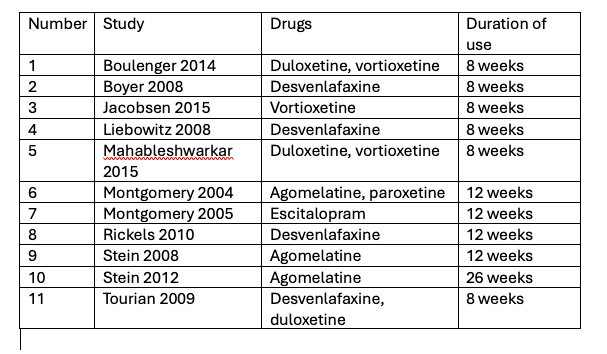
Six of these RCTs involved people exposed to antidepressants for 8 weeks, four for 12 weeks and one for 26 weeks. The 26-week trial and two of the 12-week trials looked only at agomelatine, a drug that is not known to have withdrawal effects.
Aftab does acknowledge that the majority of trials in the meta-analysis involve short-term antidepressant use (typically 8–12 weeks) - yet he still asserts that the findings challenge the narrative “that antidepressant withdrawal is very common and often severe” and his main takeaway from the paper is that “the symptom burden related to withdrawal or discontinuation for the average user of antidepressants is quite modest.”
But this sleight of hand is highly misleading and buries the significance of this issue.
As I have said before - repeatedly, apologies! - testing whether antidepressant withdrawal is common or severe for the millions of people who have been on the drugs for years or decades by examining people who have been on the drugs for 8 to 12 weeks is like a car company testing whether a car is safe on impact by crashing it into a wall at 5miles/hour and ignoring the fact that people are driving around at 60miles/hour on the roads.

Up to 4 million people in the UK have been on antidepressants for more than 2 years and about 2 million people on antidepressants in England have been taking them for over five years. In the US, at least 25 million people have taken antidepressants for more than two years. A far cry from the 8-12 week studies that the main analysis in Kalfas is based on.
Later in his piece Aftab softly adds this proviso to the interpretation that withdrawal is not significant for most people “We can say this with high confidence for short-term antidepressant treatment and with lesser confidence for long duration of antidepressant treatment.”
Aftab appears to add some nuance to this interpretation with his line but this is the same as saying: ‘the safety of car crashes at 5miles/hour in testing gives us high confidence of the safety of cars when crashing at low speeds, with lesser confidence for safety at high speeds.’
In other words, this is not nuance but nonsense.
2. Longer Use Predictably Leads to More Severe Withdrawal
Despite Aftab’s claims otherwise the notion that longer exposure increases the risk and severity of withdrawal is not speculative. It is foundational psychopharmacology. For all dependence-forming substances—from caffeine to benzodiazepines—the longer and more consistently a substance is used, the greater the neuroadaptation, and the more difficult and symptomatic the process of cessation.
Although Aftab feels he is being charitable by remaining ‘open-minded’, in fact with antidepressants, we have strong empirical data supporting this principle. Our 2025 study of over 300 patients in NHS therapy services found a clear and dramatic gradient between duration of use and withdrawal outcomes. Compared to people who had used antidepressants for less than 6 months, those who had used antidepressants for more than two years were:
· 10 times more likely to report withdrawal symptoms;
· 5 times more likely to rate those symptoms as severe;
· 18 times more likely to report long-lasting withdrawal;
· 27 times more likely to be unable to stop, despite trying.
Amongst those on antidepressants for less than six months, withdrawal symptoms were generally mild and short-lived. Three-quarters reported no or only mild symptoms, and the majority resolved within four weeks. Only one in four were unable to stop successfully when they tried to. This does not sound very different from the findings in the short-term trials focused on by Kalfas.
In contrast, for long-term users (more than two years):
• two-thirds reported moderate or severe withdrawal effects, with one-quarter reporting severe withdrawal effects.
• Almost one-third of long-term users reported symptoms that lasted for more than three months, and 11% for more than a year
• Four-fifths of these patients were unable to stop their antidepressants despite trying.
While survey-based, this study is hardly anomalous—others have found strikingly similar results. And while some critics object to survey methods, it is worth remembering that observational data are the basis for many foundational public health findings, especially related to biological gradients. We do not have RCTs showing that smoking causes cancer or that pack-years correlate with lung cancer risk. We accept these conclusions because the observational gradient is clear and plausible.
In our study, it is implausible that the dose-response gradient arose from a self-selection bias (even if the response rate was low at 18%). For that to occur, short-term users who had bad experiences would have had to systematically avoid completing the survey, and long-term users who had no problems would have had to do the same – a very unlikely state of affairs.
Aftab waves away these findings, based on the fact that no relationship between duration and withdrawal was found in the Kalfas or Henssler meta-regressions. But these regressions are underpowered and fundamentally flawed.
The Kalfas paper uses only short-term trials for its meta-regression—almost all 8 to 12 weeks—and the single 26-week study it includes is of agomelatine, a drug not associated with withdrawal. This is like analysing the height of kindergarteners and concluding height doesn’t matter for being able to dunk a basketball.

In fact, as Professor Michael Hengartner has pointed out, its actually worse than this. Kalfas report a negative association between duration of use and risk of withdrawal (that is, the longer you use a drug the less withdrawal you experience) that is almost significant. This is almost certainly because the longest study included in the meta-regression was the 26-week study with agomelatine which does not have a withdrawal syndrome, whilst the shorter studies (8 to 12 weeks) had higher risk antidepressants. This is known as the ecological fallacy – where differences between studies do not reflect the differences between individuals. This is not a credible calculation.
Similarly, the Henssler meta-analysis has been critiqued in detail in a recent article in Psychological Medicine. It relied on spontaneous adverse event reporting, included short-duration studies, misclassified adverse events, and made data extraction errors (e.g., double-counting hundreds of participants). Using Serious Adverse Events as a proxy for withdrawal severity is not a reliable approach. So the claim from this study that “duration doesn’t matter” is not supported by reliable data—and common sense tells us it is an implausible conclusion. Could it really be the case that use of an antidepressant for a week or ten years has no bearing on risk of withdrawal effects?
The Zhang et al. (2024) meta-analysis also found a dose-response relationship between treatment duration and withdrawal risk: incidence increased from 35.1% after 6–12 weeks of use to 51.4% after more than 24 weeks. While the differences were not statistically significant, probably due to being under-powered, the pattern supports the conclusion that longer antidepressant use increases the likelihood of withdrawal symptoms.
It is telling that Aftab admits, anecdotally, that he sees this gradient in his own patients.
We can be confident that longer-term users experience far more frequent and severe withdrawal than short-term users. Extrapolating from short-term trials isn’t just unreliable—it’s nonsensical. If withdrawal is ten times more likely and five times more severe after long-term use, there is no justification for applying short-term findings with even “lesser confidence.” It should not be done with any confidence at all.
3. Longer-Term Trials Show More Common and More Debilitating Withdrawal
a) The longer ANTLER study contradicts the findings of the short-term Kalfas studies
Aftab tries to reassure readers by noting that longer-term studies were included in the Kalfas review - particularly the ANTLER trial, which involved treatment durations over 36 weeks. But this reassurance is illusory.
Aftab says “[the Kalfas paper] nonetheless did have some data from studies with a long duration of antidepressant treatment, including the rigorous and high-quality ANTLER trial with a treatment duration of more than 36 weeks.”
I doubt whether Aftab has appreciated that the ANTLER study provides exactly zero data to the results section of this paper. It is included as part of ‘qualitative synthesis’ (i.e. qualitative because no numbers from this paper was used) in the supplementary material as eAppendix 5 which I re-produce here.

It is hard to understand why the authors did not report the data captured in this study in their results which does involve people who were exposed longer and therefore presents probably the most informative findings.
In ANTLER, withdrawal symptoms increased dramatically compared to the maintenance group following cessation:
· Sertraline: 4-fold increase in symptoms at 4 weeks (SMD 0.99)
· Citalopram: symptoms doubled (SMD 0.52)
· Fluoxetine: doubled (SMD 0.51)

These are large effect sizes—substantially larger than the efficacy signal for antidepressants (SMD ≈ 0.3). The data also show that withdrawal symptoms (for all antidepressants considered together) persisted and even increased at later follow-up points:
· 12 weeks: SMD = 0.6
· 26 weeks: SMD = 0.19 (new symptoms since last measurement)
· 39 weeks: SMD = 0.40 (further new symptoms since last measurement)
These figures suggest a protracted withdrawal trajectory for many patients – with symptoms present and even increasing for months after the drugs were stopped. The authors of the ANTLER study acknowledged that ‘ANTLER is therefore one of the first large “double blind” randomised controlled trial in primary care to provide evidence of withdrawal symptoms occurring over a long period after antidepressant discontinuation.’
Aftab claims that ANTLER doesn’t show people “struggling en masse” with withdrawal. But that’s not what the data show. They show worsening symptoms over time and effect sizes greater than those observed for antidepressant efficacy. It’s also worth noting that participants were allowed to restart their medication. Those who did likely had the most severe symptoms—and their withdrawal was aborted. Including them in the analysis underestimates true withdrawal incidence and severity.
ANTLER also shows that – at least for longer term users – withdrawal effects are still prominent 4 to 8 weeks after stopping the drugs, which means the 1-2 week follow-up periods employed by Kalfas are inadequate and/or that there are different timings relevant for longer term users. This is also consistent with increased recognition of delayed onset withdrawal effects where some studies find that withdrawal effects only occur weeks after drugs are stopped, also commonly seen in clinical practice.
b) Other long-term studies also find much higher rates of withdrawal than Kalfas
Aftab acknowledges the need for longer-term studies but claims they’re largely lacking. In fact, several well-conducted randomised discontinuation trials have already shown substantial withdrawal symptoms after extended antidepressant use.
Rosenbaum et al. (1998) studied discontinuation effects after 4 to 24 months of SSRI use by interrupting antidepressants for 5-8 days in 240 patients and found dramatic increases in withdrawal symptoms following abrupt cessation of sertraline and paroxetine.

On the DESS scale, discontinuation led to an average increase of 5.7 points for sertraline (effect size 0.8) and 7.8 points for paroxetine (effect size 0.9)—both substantially larger than the effects reported in the short-term trials included in Kalfas. Crucially, the study included drug continuation arms and met Kalfas’ own inclusion criteria, yet it was excluded from their main analysis. Instead, it was only used for calculating symptom-level odds ratios—a puzzling omission given the quality and relevance of the data.
Michelson et al. (2000) similarly reported high rates of withdrawal symptoms after discontinuing paroxetine and sertraline following 4 to 36 months of use. After just 5–8 days of blinded drug interruption, 57.1% of those who stopped paroxetine experienced worsening symptoms versus only 5.7% of those who continued it (p < 0.001). For sertraline, the figures were 42.4% versus 6.1% (p = 0.002).
Functional impairment was also measured: paroxetine withdrawal caused clear disruption in work, relationships, and social activity; sertraline caused impairment in overall functioning. Notably, these were short interruptions—participants were reinstated on medication after just a few days. The data give a glimpse of the severity of withdrawal symptoms that may occur or persist over weeks, months or years.
These studies directly contradict the notion that robust long-term data are lacking—and they show that longer-term use is associated with larger, more disruptive withdrawal effects than anything seen in the short-term trials Kalfas prioritised.
4. The Davies and Read Review Was Not Just Surveys
Aftab brushes off the Davies and Read 2019 review as “methodologically problematic” and implies it was reliant on low-quality surveys. But this is a mischaracterisation.
The review included both survey data and RCTs. When the analysis was restricted to just the 6 double-blind RCTs, as we did in a re-analysis in 2023 in CNS Drugs, figure below, the withdrawal incidence remained high—53.9% (not much lower than the 56% figure for the entire review). After adjusting for nocebo effects (estimated from placebo discontinuation or drug continuation arms) at 11.8%, the final estimate of withdrawal incidence was around 42%.

These findings are consistent with a 2024 systematic review led by researchers at the Chinese National Laboratory for Drug Dependence, which examined 11 RCTs and found:
· 44.4% experienced withdrawal in the discontinuation group
· 16.6% in the continuation group
· Difference = ~28%, even after short-term treatment
Notably, these studies were mostly short-term (8-12 week studies) and so these estimates only apply to shorter term studies.
And, interestingly, while the Zhang meta-analysis found evidence of a gradient for withdrawal effects in the drug discontinuation group (outlined above) it did not find a similar gradient in the nocebo group, which suggests that after long-term use the gap between withdrawal effects and nocebo effects is likely to widen even further.
Overall, it is premature of Aftab to accept the talking points that the Davies and Read review, and similar reviews do not provide robust evidence of more common withdrawal effects.
5. Even the Effects from Short-term Trials were Downplayed
In fact, whilst the results from short-term trials can’t be extrapolated well to longer term studies, even these results showed quite significant withdrawal effects after short term use.
They found the following effect sizes for the SSRI and SNRI drugs included in the analysis:
· desvenlafaxine (g=0.39),
· duloxetine (g=0.40),
· escitalopram (g=0.43), and
· paroxetine (g=0.68)
These do not seem like trivial effects, especially when this class of antidepressants has been approved on achieving an effect size of g=0.3 in terms of improvement in depression scores. The effect size for withdrawal is larger than the antidepressant effect for each of the antidepressants listed above.
There was a decrease in effect after two weeks (g=0.13) but this shows that not all withdrawal symptoms remit within two weeks after just 8 to 12 weeks of antidepressant exposure.
Similarly large effects for individual symptoms are summarised by Aftab, without acknowledging their implications:
Dizziness: OR 5.52
Vertigo: OR 6.40
Nausea: OR 3.16
Nervousness: OR 3.15
He calls this “not particularly news to most practicing psychiatric clinicians.” But these are large odds ratios, suggesting that certain symptoms—some of which can be disabling—are multiple times more likely after antidepressant cessation than placebo, even after short-term use (since most trials were short term).
And notably antidepressants were found to have an OR of between 1.4 and 2.1 in antidepressant ‘response’. So this means that withdrawal effects are two- or even three-fold more likely to occur than antidepressant effects from these drugs - not to be brushed off.
6. The DESS Score Is Not a Measure of Severity or Harm
Aftab acknowledges that the Discontinuation-Emergent Signs and Symptoms (DESS) inventory, the main outcome used in the meta-analysis, does not measure symptom severity. Yet he still concludes that “the symptom burden related to withdrawal or discontinuation for the average user of antidepressants is quite modest,” based on the finding that patients experience one more symptom on average than placebo.
As Aftab himself quotes from the supplementary materials: “An increased DESS score may not reflect severity.”
The DESS awards one point each to “dizziness,” “agitation,” and “insomnia,” with no weighting, duration, or functional impact assessed. As Aftab suggests, one patient may report three mild symptoms; another may experience a single, incapacitating one—but both receive similar scores.
To infer from this that withdrawal is “modest” is like measuring earthquakes by the number of tremors rather than their magnitude. The conclusion does not follow from the data. And as shown above from Michelson (2000) after a few days of withdrawal people were already having work, relationship and overall problems functioning. Imagine what weeks, months or years of these sort of symptoms might produce.
7. No, Depressed Mood After Stopping Antidepressants Cannot Simply Be Assumed to Be Relapse (Aftab got this right)
One of the most problematic claims in the Kalfas meta-analysis - and one where Aftab, to his credit, is highly skeptical - is the suggestion that withdrawal “was not associated with depressive symptoms,” implying that post-discontinuation depression reflects relapse rather than withdrawal.
Kalfas argues that the later return of depressive symptoms “is indicative of depression relapse,” because it was not detected as a withdrawal symptom in their analysis. But this conclusion rests on just five trials—many of which relied on spontaneously reported adverse events, a method known to vastly under-detect withdrawal symptoms compared to structured instruments.
Aftab counters this view, telling of patients he’s seen who have developed rapid and severe depression with suicidality on stopping antidepressants - nothing like anything they’ve experienced before, clearly marking it as a withdrawal effect. I have seen or heard from hundreds of similar patients (indeed, I was lucky enough to be one) – who were put on antidepressants following the loss of a loved one, divorce, work stress, with moderate symptoms - who have developed akathisia or severe and debilitating symptoms nothing like the symptoms that put them on the drugs in the first place, as we captured in our survey here.
But we do not need to rely on anecdote alone because in contrast to Kalfas, better-designed studies using systematic assessment show a different picture with depression arising as a clear withdrawal effect. In Rosenbaum et al. (1998), after abrupt discontinuation of antidepressants for 5–8 days:
The Hamilton Depression Rating Scale (HDRS) increased by:
−0.1 for fluoxetine (which can be considered as a control due to its long half-life)
+3.5 for sertraline
+5.6 for paroxetine
These changes in depressive symptoms closely mirrored changes in withdrawal scores, as measured by the DESS:
Fluoxetine: −1.8
Sertraline: +2.9
Paroxetine: +8.25
You can see this in the figure re-produced from a 2022 study where we analysed the Rosenbaum data (DESS = withdrawal score, MADRS/HRSD = depression score; ‘Before’ drugs were stopped, ‘During’ 5-8 days of cessation and ‘After’ re-instatement of the drug).
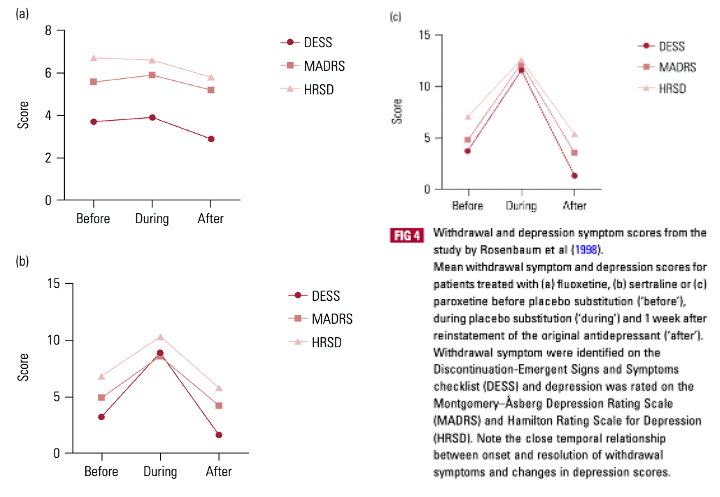
Moreover, when the antidepressants were reinstated, both the depression and withdrawal scores returned to baseline. This is classic withdrawal: the timing (within days of cessation), the pattern (mirroring withdrawal intensity), and the resolution (disappearing with drug reinstatement) all confirm it.
Some may argue that this could reflect both relapse and withdrawal. But applying Occam’s Razor—a core principle in clinical reasoning—it’s far more parsimonious to conclude that one cause (withdrawal) is producing multiple symptoms, rather than assuming two independent syndromes coincidentally occurred at the same time and resolved simultaneously. Given the probabilities of relapse and withdrawal it is much more likely that symptoms experienced after stopping antidepressants are withdrawal rather than relapse.
Rosenbaum also calculated how many participants would have met standard relapse thresholds (HDRS >8):
6% for fluoxetine
30% for sertraline
36% for paroxetine
These figures are vastly higher than the 1.3% rate of “post-discontinuation depression” reported by Kalfas, highlighting how flawed their method was for detecting depressive symptoms.
In fact, the sertraline ‘relapse rate’ in Rosenbaum (the proportion of participants who would have fulfilled standard criteria for relapse) is higher than the entire relapse difference between continuation and discontinuation groups in the ANTLER trial—suggesting that what is often labelled as “relapse” in these studies may in fact be misclassified withdrawal.
The notion that stopping antidepressants can cause depressed mood that is not just a return of an underlying condition is also supported by a survey we conducted in more than 1000 people who had experienced withdrawal effects from their antidepressants. Respondents were as likely to report depressed mood on stopping the drugs whether they were prescribed the antidepressant for a mental health condition or a physical health condition.
And while 57% of the sample reported depressed mood before starting antidepressants (with severity on average 1.02 out of 3, where 0= no symptoms, and 3= severe symptoms), 93% reported depressed mood after (or during tapering) stopping (with severity 2.23 out of 3). In other words, many people experienced depressed mood de novo from antidepressant withdrawal and it was more severe than the underlying condition.
So it is not justifiable to conclude from the Kalfas data that depressive symptoms after stopping antidepressants are relapse rather than withdrawal. This kind of messaging has led to widespread misdiagnosis, unnecessary re-prescribing, and prolonged suffering for patients. Repeating this misleading message only perpetuates the problem.
8. The Drugs Most Known for Causing Withdrawal Were Underrepresented
Aftab admits that drugs like paroxetine and venlafaxine, long known to be the most withdrawal-prone, were poorly represented in the Kalfas dataset. Yet he still extrapolates the “modest” withdrawal effect to the general antidepressant-using population.
This is unjustified. You cannot generalize from data that excludes the worst offenders. He notes that agomelatine, which has no known withdrawal profile, was included multiple times, further diluting any signal of harm.
This selective sampling produces a misleading average and minimizes the very cases that matter most in clinical practice.
9. The Central Problem Remains: There are still not safe tapering studies
To Aftab’s credit, he highlights what should be the real scandal:
“It’s a travesty that nearly four decades after the approval of Prozac, there’s not a single high-quality randomized controlled trial that can guide clinicians in safely tapering patients off antidepressants.”
Exactly. That absence of evidence is the real context in which withdrawal needs to be understood. We are dealing with a common, distressing, sometimes disabling syndrome that has been woefully understudied, and Kalfas et al. do not change that. They simply show us how little we’ve been looking.
Conclusion: The Wrong Takeaway
The Kalfas meta-analysis is being used by Aftab—and will undoubtedly be used by others—as evidence that concerns about antidepressant withdrawal have been overstated by patient communities and critics of mainstream psychiatry. But that is the wrong conclusion to draw.
What the study actually shows is that even after short-term use (8 to 12 weeks), SSRIs and SNRIs produce clear and measurable withdrawal symptoms—often with effect sizes larger than the drugs’ own efficacy in short-term trials (SMD ≈ 0.3). These are not trivial findings.
However, the trials included in Kalfas almost exclusively reflect short-term treatment. They cannot be extrapolated to the millions of people who have taken antidepressants for years, because we have compelling evidence—from observational studies, some meta-regressions and basic pharmacology—that longer-term use results in much more frequent, more severe, and more persistent withdrawal symptoms.
Several high-quality discontinuation studies after long-term antidepressant use have reported withdrawal rates two to three times higher than those found in short-term trials, with functional impairment emerging within just days of cessation. Trials like ANTLER show that withdrawal symptoms not only emerge but persist for months after stopping. Surveys of long-term users further suggest that severe symptoms are common, particularly in those who have taken antidepressants for over two years.
Taken together, this is not a reassuring picture. The real takeaway is that millions of people are at risk of severe and enduring withdrawal symptoms and many of them are stuck on drugs they would like to stop but can’t. Rather than minimising these concerns, psychiatry should be investing in safe tapering strategies, providing proper support for those in withdrawal, and taking urgent action to limit unnecessary long-term prescribing—so that fewer people are harmed in the first place.
----
I’ll just add here – and this is not in response to Aftab, but to the authors of the Kalfas paper itself – that I consider myself a pretty jaded, cynical person but I was shocked at the senior authors of the Kalfas paper calling for their review – despite all the limitations outlined above, and even by Aftab – to lead to an update to guidelines, to reflect that withdrawal was not a significant problem.
The senior author, Dr Sameer Jauhar, in the official press release from King’s College London and Imperial College London explicitly projected an undeservedly reassuring message to the public. He said: “Despite previous concern about stopping antidepressants, our work finds that most people do not experience severe withdrawal, in terms of additional symptoms.” No indication that this was based on very short-term studies.
Professor Allan Young went further, saying: “Now, this cutting-edge review clarifies the scientific evidence and should reassure all parties about the use, and discontinuation, of these treatments. Official guidance should now be changed to reflect the evidence.”
This is a call to update national guidelines to indicate that withdrawal is not a significant problem – guidelines that inform GPs, psychiatrists, pharmacists and other professionals who care for patients around the country, some of whom have been on antidepressants for years or decades.
There is already a widespread issue with clinicians not being well-informed about withdrawal effects leading to mis-diagnosis when people present with severe issues, leading to unnecessary suffering and sometimes drastic consequences. Winding back the small progress that has occurred in guidelines over the last few years would exacerbate this already dire problem. Professor Young was one of the academics involved in Eli Lilly’s original symposium in the 1990s to spread the term ‘discontinuation symptoms’ and the message that these were ‘brief and mild’. It looks like decades later his dedication to this message has not waned. I sincerely hope that guideline committees are not taken in by this unwarranted call based on short-term evidence.
Thank you Mark. This is a very helpful analysis of where we are.
I respect Awais Aftab very much. However, his recent commentary on antidepressant withdrawal, following the publication of the JAMA Psychiatry paper, left me concerned.
I am not a researcher but I am well versed in much of the scientific literature in relation to antidepressant withdrawal. I remain concerned that lived experience of withdrawal is considered of lesser value by psychiatry as a profession than short-term, largely pharma-sponsored studies.
The Science Media Centre's involvement [approach to] the worldwide distribution of the JAMA Psychiatry is also of concern. The BMJ followed the SMC briefing and uncritically broadcast the views of career-long paid opinion leaders such as Prof Allan Young. The BMJ later had to amend their News article on this. Something is wrong here.
Great critique, Mark!